WAM was developed as Unit 9 of the BA Product & Industrial Design programme at Central Saint Martins (UAL), submitted January 2022. The brief opened broadly — a sensor-driven assistive system for older adults — and narrowed through user-research and clinical literature to the single intervention with the strongest evidence base: preventative strengthening before muscle weakness compounds into instability.
Preventative, not reactive.
01 / PROBLEMReactive devices treat the consequences of a fall; the outcome data justifies acting earlier. Within one year of a hip fracture, 20% of patients die from complications and around 50% become permanently disabled. The single most effective intervention identified in the source literature is participation in a structured strength-and-balance exercise programme — a target WAM is built to support rather than replace.
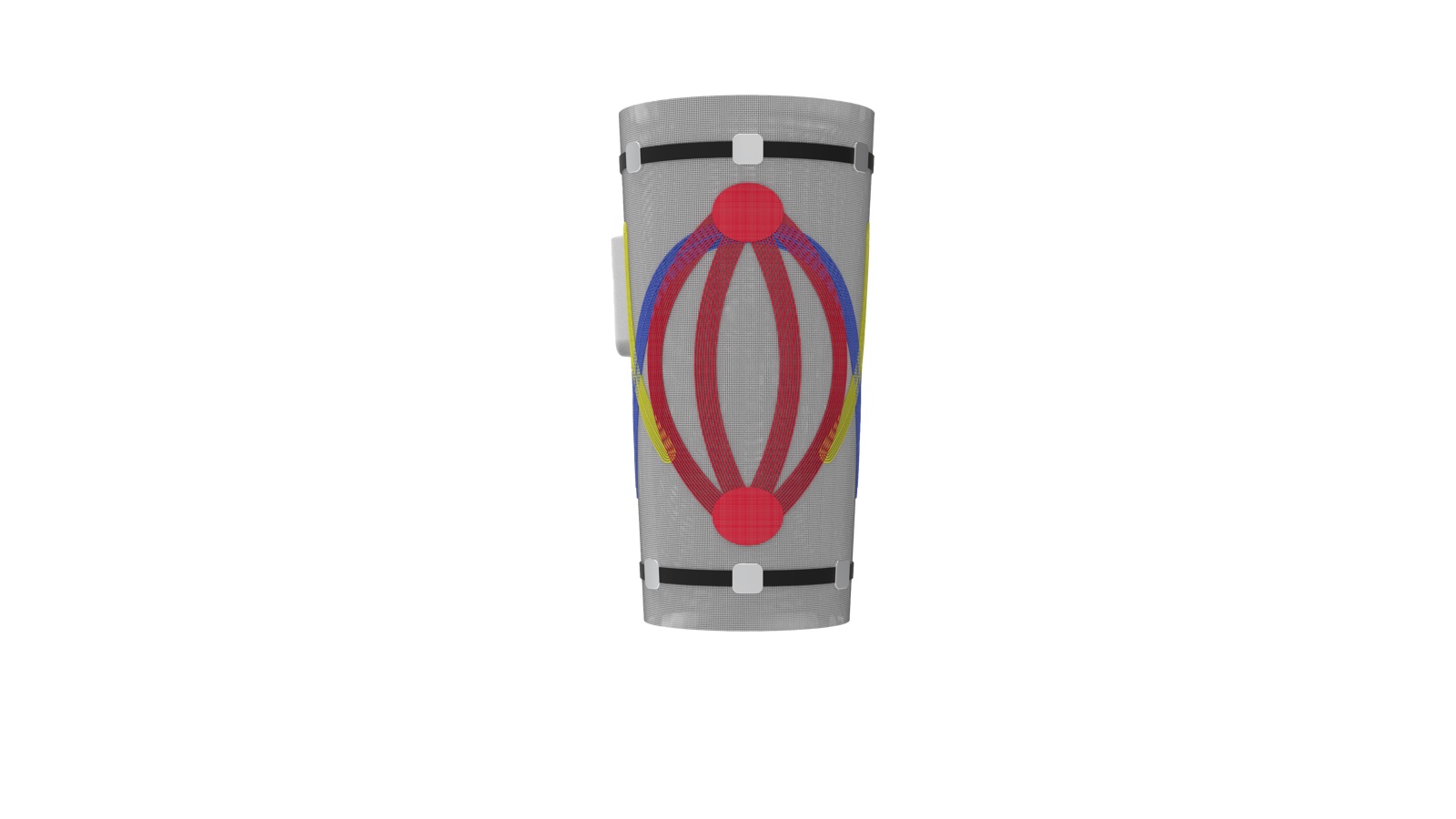
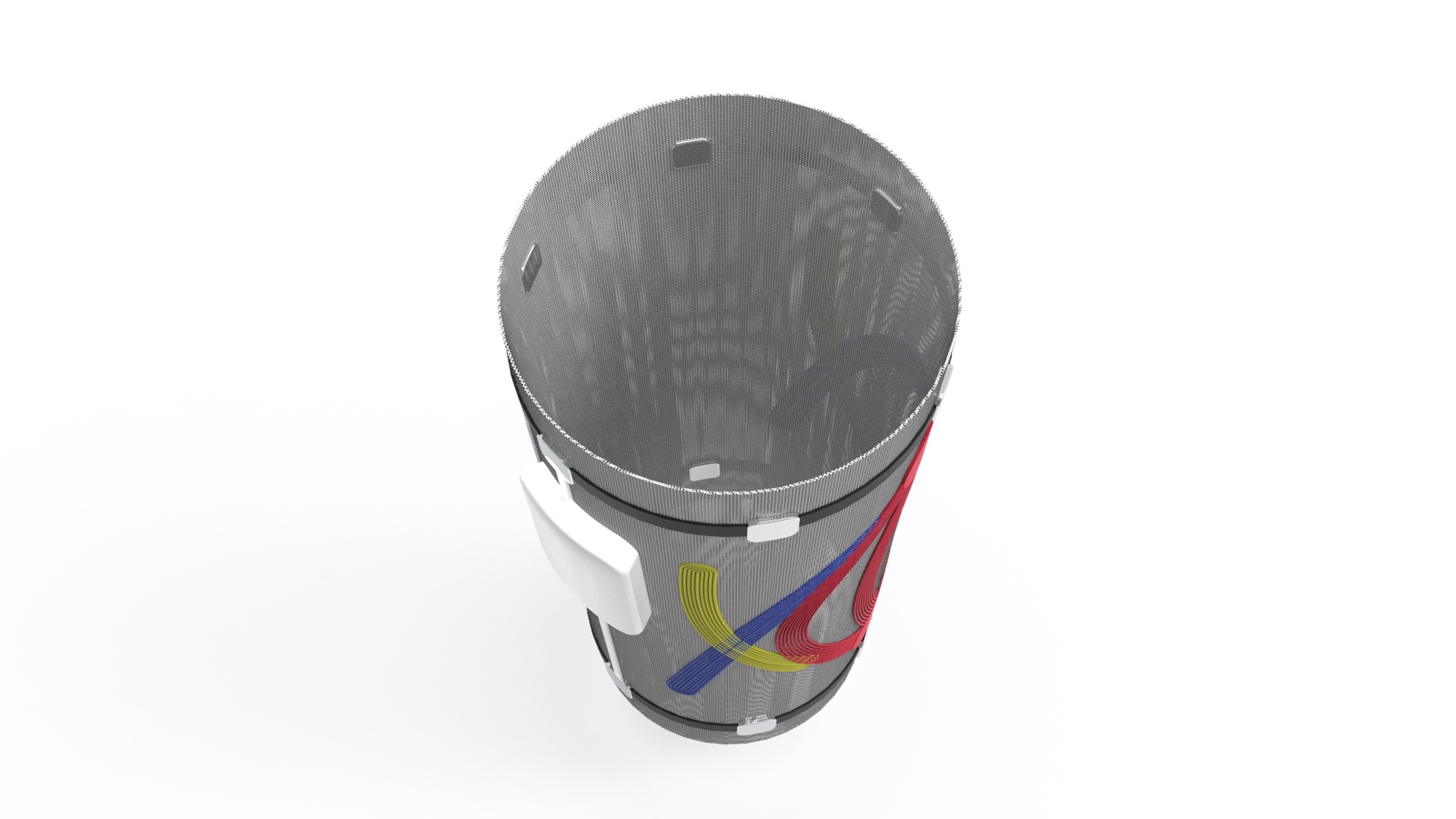
WAM is a knee-worn device that pairs surface EMG with a connected support structure. Sensors monitor muscle activity on the wearer; the data feeds a companion app that surfaces weakness trends to both the wearer and their supervising physiotherapist; embedded support structures in the knit deliver targeted reinforcement informed by that data, adjustable as recovery progresses.
Construction & technical approach.
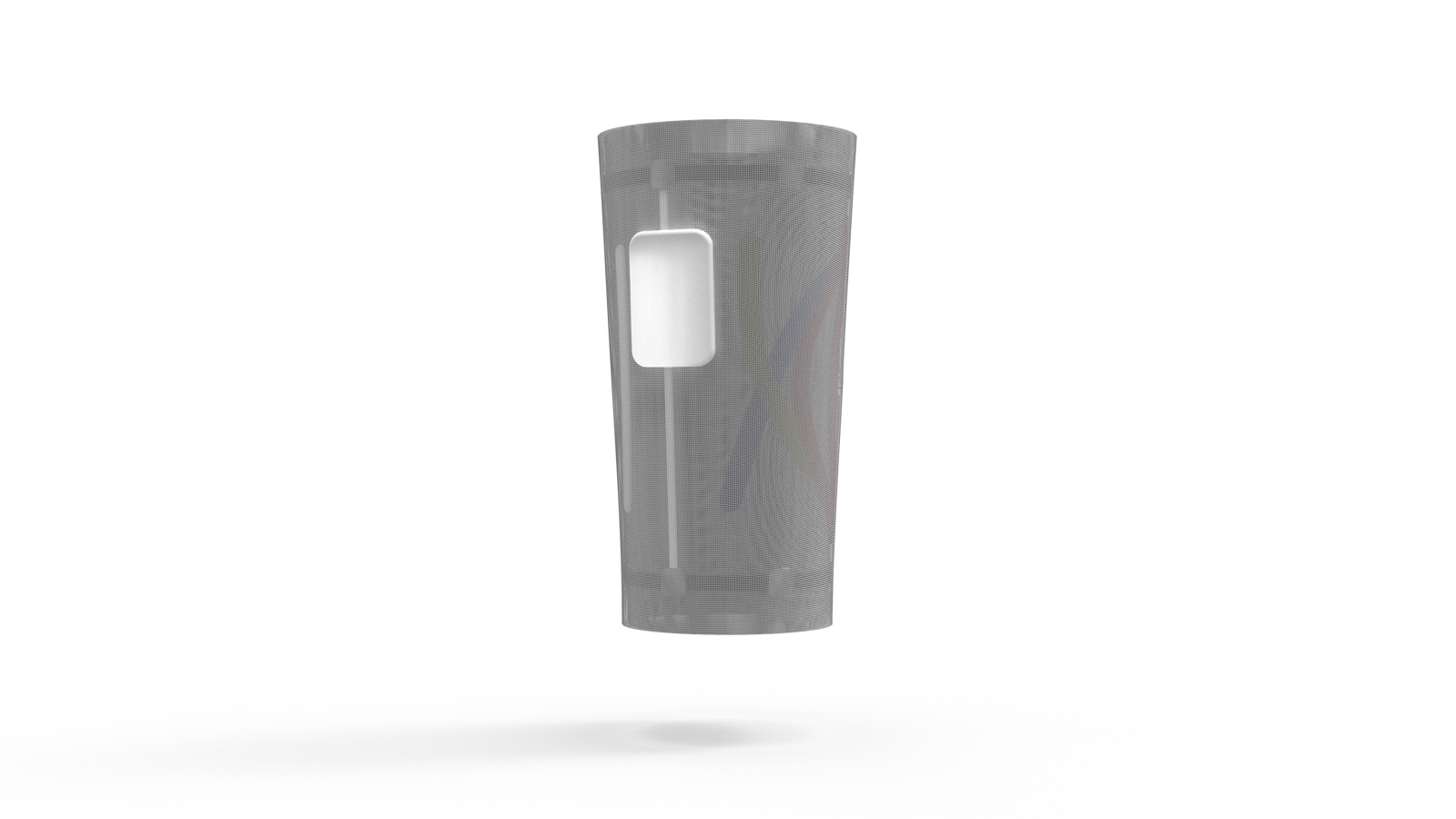
02 / METHODThe construction is a three-layer knit: a compression base, a support mid-layer integrating tensile fibres and inflatable channels as secondary muscle elements, and an outer Flyknit-style sock layer providing structural support without reading as medical equipment. The technology stack synthesises four reference points: Nike Flyknit (sock-fit support fabric), Uniqlo’s WHOLEGARMENT 3D-knit machine (one-piece manufacture), Thalmic Labs’ MYO controller (wearable EMG signal acquisition, the same sensing principle WAM uses for the leg), and KT-tape kinesiology pathways (muscle-support routing). The cycling-helmet airbag Hövding sits in the reference set as a precedent for protective wearable tech disguised as an everyday garment.
Three design variations were prototyped and compared: external supporting fibres, external printed silicone, and embedded supporting fibres. The embedded-fibre variant was selected for final development. A bespoke physical prototype was constructed with a sourced tailor — two knee sleeves stitched together to demonstrate the three-layer structure, with EMG sensors and the main circuit board integrated on the outer face and KT-tape muscle-support pathways routed across the mid-layer.
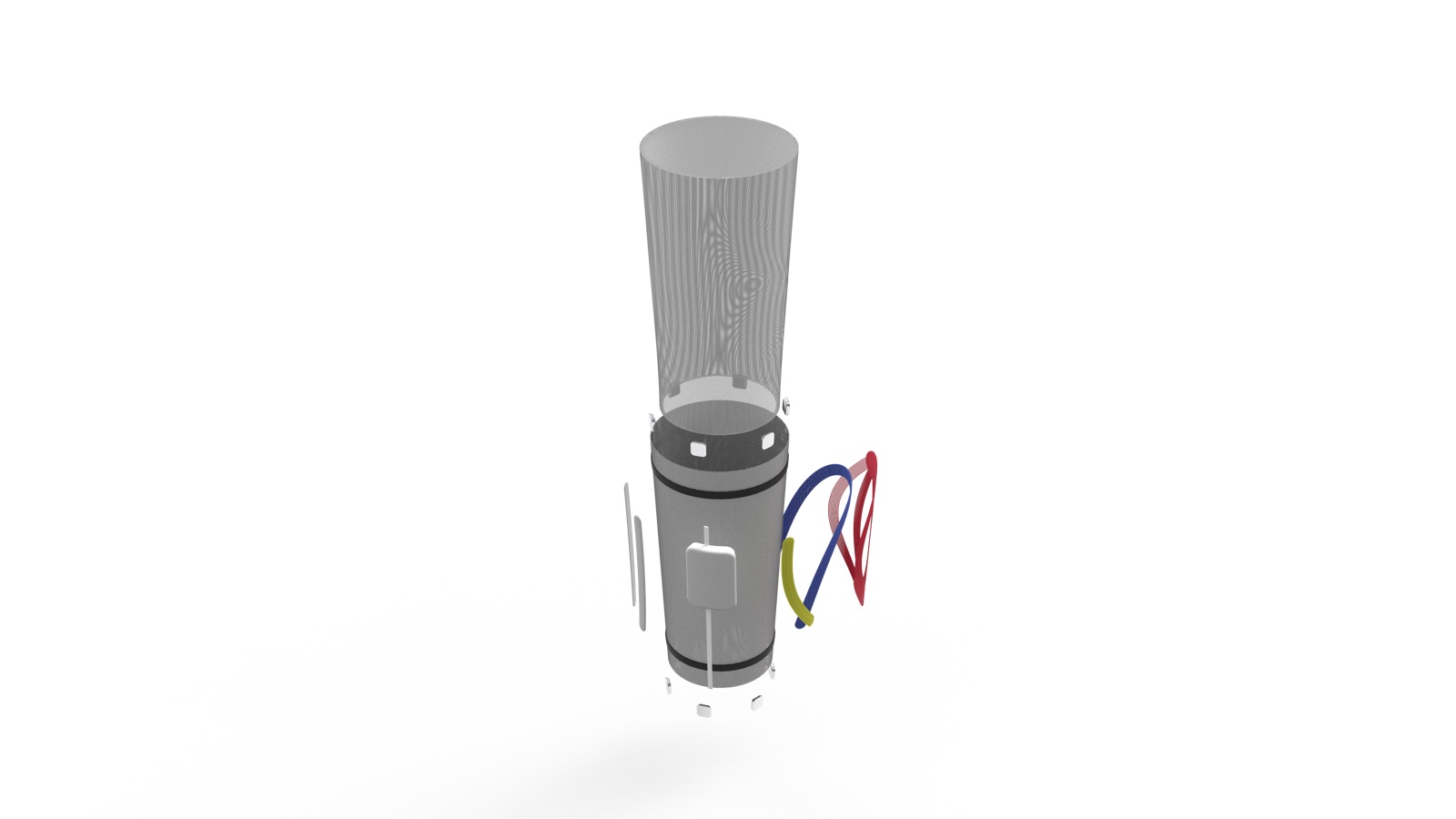
The final assembly comprises eleven engineered components: outer fabric layer, upper and lower EMG sensors with cables, four support structures (back, side, front, knee), a circuit board housed in injection-moulded recycled plastic, and an inner fabric layer. Fabric materials (cotton, polyester, nylon, rubber blends) were specified for recyclability where the textile lifecycle allowed; the circular pathway through the moulded electronic components remains a known limitation flagged for further development.


Outcome.
03 / RESULTWAM began with a broad open-ended care brief and narrowed via user research and clinical literature into a single defensible intervention. The harder discipline was deciding which constraint to honour as a design input rather than a limitation — accepting EMG’s noise floor, accepting the textile recycling boundary, accepting the physiotherapist’s existing workflow — and treating each as part of the brief, not a finishing layer.
It set the working approach that runs through every project since: engineering specificity over conceptual gesture, manufacturer and supplier reality treated as a design input from day one, and stakeholder-side reasoning — a clinician’s workflow, a wearer’s daily routine — folded into the brief rather than retrofitted at the end.